
Anxiety and Psychosomatics: how to work with your clients – Applied Integrative Sciences #1
Jan 03, 2022In this article we start to present a series of practical case studies to understand how to work in practical terms and get the most out of the Integrative Sciences and its schemes, models, techniques and application strategies.
We will present real case studies, with a targeted selection of the most relevant phases, factors and techniques. It will thus be possible to gradually become familiar with an articulated system that presents different possibilities for intervention.
This first case study is featured in The Science of Psychotherapy magazine (October 2019), you can download a copy from this link or read the article below.
CASE 1
Let us look at a first practical example to understand how these models and the Applied Integrative Sciences can help us and our patients to include different elements of analysis and practice right away. Let us start with a simple case of limited scope and gradually broaden our perspective:
an anxious patient with typical cervical spine and/or lower spine somatisation symptoms. In this instance, we can use the Switch model and start from the top by focusing on the mental, creative, physical and postural flows that are involved.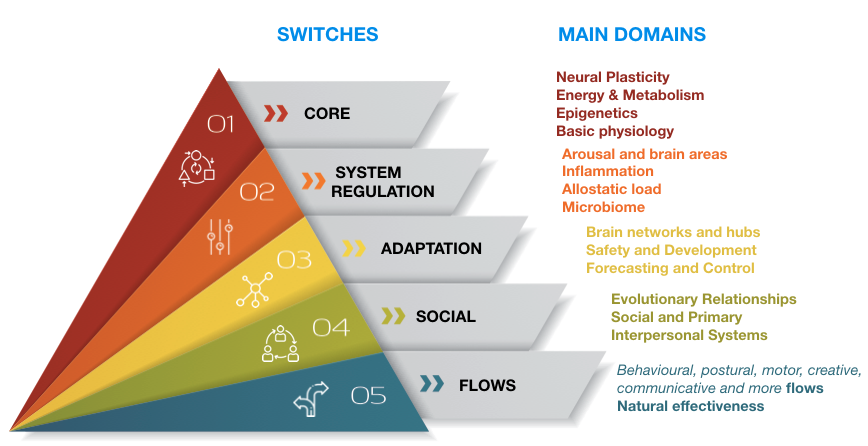
Let us focus a moment on a detail, among a variety of elements we could analyse, that is under-investigated by most psychotherapeutic methods, even when they are based on the body. This detail is an aspect on which it is critical to intervene to ensure efficient outcomes: it is the analysis of the functional anatomy of movement in a stress response and the understanding of how to manage it starting with muscle tone.
In our example it is important to explain to the patient how biomechanical movement caused by their chronic adaptation response leads to their postural problem: if the diaphragm shortens and remains contracted longer than necessary the neck and lumbar curves increase, and the head moves forwards to compensate.
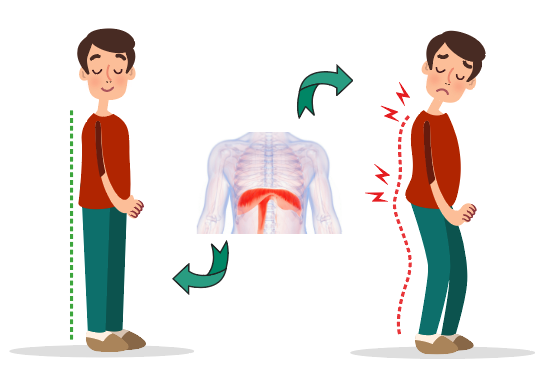
When looked at side-ways, a person’s cervical spine should be aligned with the shoulder blades and tailbone.
In the studios where I give consultations there is always an area that is free of furniture and pictures. You can now understand why this is: I need this area because, in cases like this one, I often suggest that my patients rest their back against the wall: first of all the tailbone adheres to the wall, then the shoulder blades and, in cases such as this one, the head is always a few centimetres (if not much more) further ahead!
During workshops I always ask participants to think about their studios and identify the ugliest picture in them… it’s the one they could remove to free up a portion of wall to use in this, but also in many other techniques.
The further away the head is from the wall, the more stressed the person is. This simple empirical measurement is very effective because the patient is able to physically perceive their lack of physiological state.
“Feeling the body” is a critical element of the switch area n.3 where we encounter different brain networks that are key to our self-regulation. One of these for example is the Salience Network in which the insula evaluates physical resources available pitting them against a specific problem. In this case we can make a note on our sheet to remind ourselves to return to this area and carry out further ad hoc techniques and evaluations such as leveraging slow movements and during the negative phase those of larger muscles that help the insula in its work on awareness processes relating to available resources (Resource Balance techniques).

Worksheet example 1
In cases such as this one – in order to favour the integration between postural flows (switch area n.5), awareness (n.3) and the meta-perception of the self and social image (n.4) – I also introduce activity including the use of cameras and video recordings that represent an excellent meta-cognitive and objective assessment element that patients can compare with their own perceptions. These are highly efficient methods that engage the patient making them play a more active part in therapy.
In some of our research we have seen very clearly that over time reducing stress via life choices (such as changing profession) or through deep psychotherapy, the distance between head and wall can be reduced a little as a result of the top-down release of the diaphragm (in other words the mind relaxing the body and benefiting from it too). On the other hand, if you combine psychotherapy/counselling sessions with a technique that intervenes directly on the somato-emotional release of the diaphragm and the muscle chains involved in the process, recovery is far more rapid and consistent.
![]()
To achieve this we suggest the introduction of a targeted technique such as Crossed Cycles Breathing that can restore physiological balance in stress responses while at the same time provide relief to the cervical spine and tailbone area thanks to movements of the head that are combined with breathing phases.
At a later stage, when the physical part of the exercise starts to be assimilated, you can include some variations and combine some danger-and-resource analysis work, always being careful to maintain awareness of all elements at play in the brain networks that manage them.
In the previous example we only considered some of the elements present in areas 3, 4 and 5. Our analysis can – and must- proceed still further.
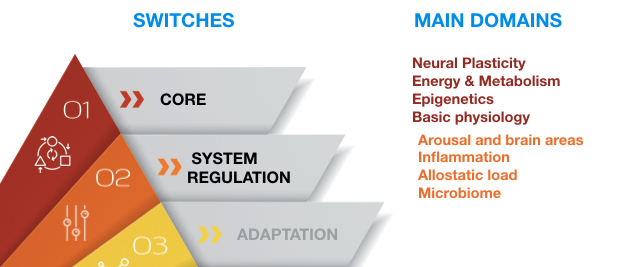
In areas 1 and 2 we find primary elements in terms of complexity and functional hierarchies. For example, in 2002 the American Psychiatric Association Task Force on DSM-IV officially highlighted that is it is possible to encounter an inflammatory state and metabolic dysregulation in any pathology or pathological dysfunction. The food that we eat every day, and in particular sugars that mobilise insulin, play a key role as cause – or at least as concurring element – that significantly amplifies anxiety and stress symptoms.
Just a few years ago there was little awareness of this fact, but nowadays we could even call it an epidemic as most of the western population presents a state of chronic inflammation and almost all the adult population presents markers for persistent subclinical inflammatory states combined with physical and/or mental issues.

We have introduced a series of questions to our first interview with the patient that are based on the Switches model and that relate to lifestyle, nutrition habits, circadian rhythms and other elements that significantly alter metabolism and inflammatory states. These are all conditions that can easily be verified through a routine blood test.
Via a few simple expedients connected to physical activity and exposure to natural light – or on the other hand – to the reduction of blue light exposure as from digital devices, the reduction of sugar and protein intake and a series of other elements, patients start to feel a significant improvement in mood and available energy even when they are not also undertaking specific therapy within 3-4 weeks. When these actions are undertaken alongside initial treatment phases, compliance increases and resistance to change decreases.
These results are the fruit of lengthy research and are easy to understand when you consider the underlying neurobiological processes. Inflammatory states amplify emotional and defensive responses as shown by all studies on PTSD and chronic stress. A hyperactive system avoids danger and is not open to change. In addition to this, inflammation erodes the neural network, while change and learning require plasticity and energy to thrive.
Restoring these favourable conditions is the first step to achieving the foundations of change which sets the scene for all later techniques and interventions.
Stay connected with news and updates!
Join our mailing list to receive the latest news and updates from our team.
Don't worry, your information will not be shared.
We hate SPAM. We will never sell your information, for any reason.
